In many cases, even a severely compromised tooth can be retained with endodontic treatment. In the case of resorptive defects, we employ both surgical and non-surgical approaches with the goal of preserving the natural dentition.
Treatment
Resorption can occur as a single entity, or a combination of internal and external defects can occur simultaneously on the same tooth. Effective management and appropriate treatment can only be carried out if the true nature, history, and exact location of the resorptive defect are known.
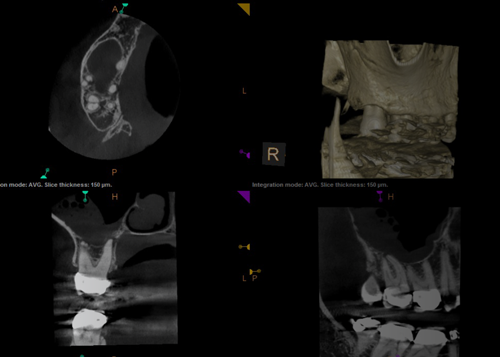
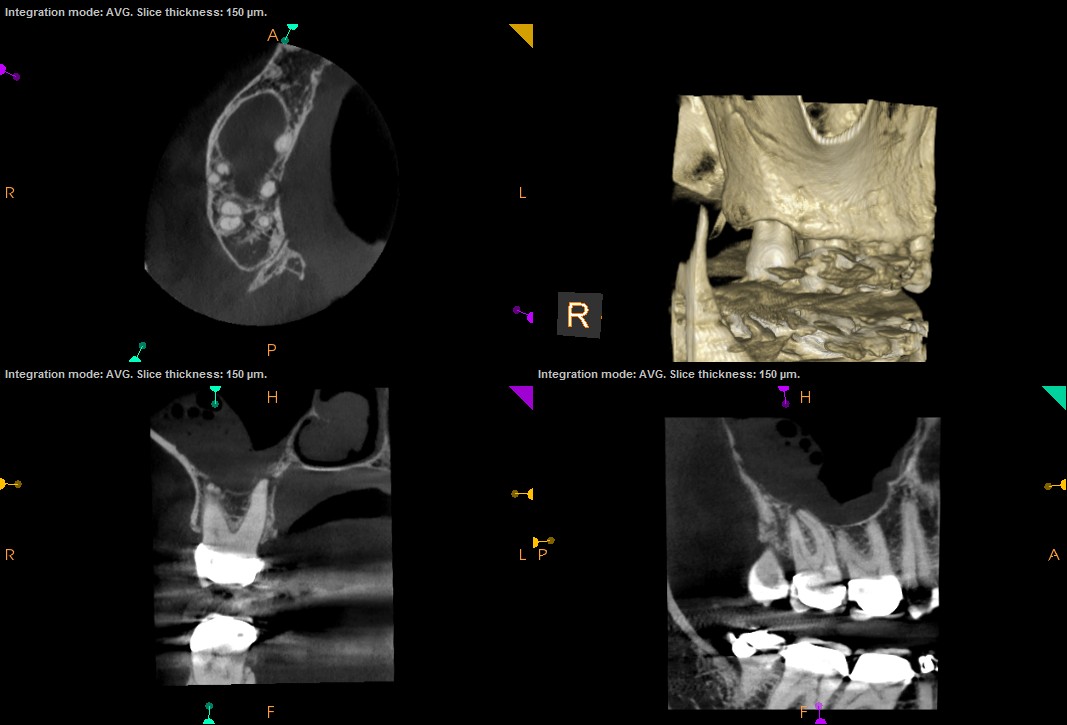 Cone Beam Computed Tomography (CBCT) has been shown to be an important adjunct for the diagnosis and treatment of resorptive defects.
Cone Beam Computed Tomography (CBCT) has been shown to be an important adjunct for the diagnosis and treatment of resorptive defects.
Internal vs. External Resorption
The following diagnostic features can often help distinguish internal from external resorption in clinical practice:
Internal
- An internal resorptive lesion appears to be close or continuous with the pulp whatever the angle of the x-ray.
- In internal resorption, the outline of the canal is often distorted and the canal and resorptive defect are contiguous.
- Internal resorption is rarely accompanied by bone loss around the tooth.

Internal: Original site of resorption starts in the pulp.

External: Original site is the periodontal ligament.
External
- An external resorptive lesion typically moves away from the canal as the angle of the radiograph changes. In addition, the buccal object rule can often help distinguish if the defect is on the buccal or lingual.
- When a resorptive defect is external, the root canal outline appears to be normal and can often be seen running through the defect.
- External resorption is frequently accompanied by bone loss around the tooth.